%22%20fill=%22%23FFFFFF%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22Shape%22%20points=%2220%209.52380952%2010.4761905%209.52380952%2010.4761905%200%209.52380952%200%209.52380952%209.52380952%200%209.52380952%200%2010.4761905%209.52380952%2010.4761905%209.52380952%2020%2010.4761905%2020%2010.4761905%2010.4761905%2020%2010.4761905%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cg%20id=%22Make-an-Enquiry%22%20transform=%22translate(25.184000,%2087.328000)%22%20fill=%22%23FFFFFF%22%20fill-rule=%22nonzero%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22M%22%20points=%229.184%2010.672%2010.784%2010.672%2010.784%200%208.496%200%205.392%207.664%202.288%200%200%200%200%2010.672%201.6%2010.672%201.6%202.192%205.056%2010.672%205.728%2010.672%209.184%202.192%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M17.888,10.672%20L19.328,10.672%20L19.328,5.456%20C19.328,3.488%2017.904,2.752%2016.224,2.752%20C14.976,2.752%2013.92,3.168%2013.056,4.016%20L13.68,5.008%20C14.368,4.32%2015.12,3.984%2016,3.984%20C17.104,3.984%2017.888,4.56%2017.888,5.52%20L17.888,6.8%20C17.296,6.112%2016.4,5.776%2015.36,5.776%20C14.064,5.776%2012.672,6.544%2012.672,8.304%20C12.672,10%2014.08,10.864%2015.36,10.864%20C16.4,10.864%2017.28,10.496%2017.888,9.824%20L17.888,10.672%20Z%20M17.888,8.976%20C17.456,9.552%2016.704,9.856%2015.904,9.856%20C14.864,9.856%2014.128,9.232%2014.128,8.32%20C14.128,7.408%2014.864,6.784%2015.904,6.784%20C16.704,6.784%2017.456,7.088%2017.888,7.664%20L17.888,8.976%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22k%22%20points=%2226.816%2010.672%2028.64%2010.672%2025.28%206.448%2028.608%202.944%2026.8%202.944%2023.072%206.864%2023.072%200%2021.632%200%2021.632%2010.672%2023.072%2010.672%2023.072%208.528%2024.24%207.344%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M29.472,6.8%20C29.472,9.232%2031.168,10.864%2033.472,10.864%20C34.72,10.864%2035.808,10.464%2036.576,9.712%20L35.904,8.768%20C35.328,9.36%2034.432,9.68%2033.616,9.68%20C32.064,9.68%2031.104,8.592%2030.992,7.28%20L37.104,7.28%20L37.104,6.928%20C37.104,4.56%2035.664,2.752%2033.344,2.752%20C31.088,2.752%2029.472,4.56%2029.472,6.8%20Z%20M33.344,3.936%20C34.976,3.936%2035.664,5.216%2035.696,6.24%20L30.976,6.24%20C31.056,5.184%2031.792,3.936%2033.344,3.936%20Z%22%20id=%22e%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M47.808,10.672%20L49.248,10.672%20L49.248,5.456%20C49.248,3.488%2047.824,2.752%2046.144,2.752%20C44.896,2.752%2043.84,3.168%2042.976,4.016%20L43.6,5.008%20C44.288,4.32%2045.04,3.984%2045.92,3.984%20C47.024,3.984%2047.808,4.56%2047.808,5.52%20L47.808,6.8%20C47.216,6.112%2046.32,5.776%2045.28,5.776%20C43.984,5.776%2042.592,6.544%2042.592,8.304%20C42.592,10%2044,10.864%2045.28,10.864%20C46.32,10.864%2047.2,10.496%2047.808,9.824%20L47.808,10.672%20Z%20M47.808,8.976%20C47.376,9.552%2046.624,9.856%2045.824,9.856%20C44.784,9.856%2044.048,9.232%2044.048,8.32%20C44.048,7.408%2044.784,6.784%2045.824,6.784%20C46.624,6.784%2047.376,7.088%2047.808,7.664%20L47.808,8.976%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M56.768,10.672%20L58.208,10.672%20L58.208,5.248%20C58.208,3.616%2057.36,2.752%2055.728,2.752%20C54.528,2.752%2053.504,3.408%2052.992,4.032%20L52.992,2.944%20L51.552,2.944%20L51.552,10.672%20L52.992,10.672%20L52.992,5.152%20C53.408,4.576%2054.224,4.032%2055.12,4.032%20C56.112,4.032%2056.768,4.448%2056.768,5.728%20L56.768,10.672%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22E%22%20points=%220%2034.672%207.168%2034.672%207.168%2033.264%201.6%2033.264%201.6%2029.936%207.056%2029.936%207.056%2028.528%201.6%2028.528%201.6%2025.408%207.168%2025.408%207.168%2024%200%2024%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M14.352,34.672%20L15.792,34.672%20L15.792,29.248%20C15.792,27.616%2014.944,26.752%2013.312,26.752%20C12.112,26.752%2011.088,27.408%2010.576,28.032%20L10.576,26.944%20L9.136,26.944%20L9.136,34.672%20L10.576,34.672%20L10.576,29.152%20C10.992,28.576%2011.808,28.032%2012.704,28.032%20C13.696,28.032%2014.352,28.448%2014.352,29.728%20L14.352,34.672%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M25.024,37.616%20L25.024,26.944%20L23.584,26.944%20L23.584,28.048%20C23.008,27.28%2022.08,26.752%2021.04,26.752%20C19.024,26.752%2017.6,28.272%2017.6,30.8%20C17.6,33.328%2019.024,34.864%2021.04,34.864%20C22.048,34.864%2022.96,34.4%2023.584,33.552%20L23.584,37.616%20L25.024,37.616%20Z%20M23.584,32.448%20C23.184,33.056%2022.304,33.584%2021.44,33.584%20C20,33.584%2019.104,32.416%2019.104,30.8%20C19.104,29.2%2020,28.032%2021.44,28.032%20C22.304,28.032%2023.184,28.544%2023.584,29.168%20L23.584,32.448%20Z%22%20id=%22q%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M32.528,34.672%20L33.968,34.672%20L33.968,26.944%20L32.528,26.944%20L32.528,32.496%20C32.096,33.072%2031.28,33.584%2030.384,33.584%20C29.392,33.584%2028.752,33.2%2028.752,31.92%20L28.752,26.944%20L27.312,26.944%20L27.312,32.4%20C27.312,34.032%2028.128,34.864%2029.776,34.864%20C30.96,34.864%2031.936,34.256%2032.528,33.616%20L32.528,34.672%20Z%22%20id=%22u%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M36.96,25.648%20C37.472,25.648%2037.888,25.248%2037.888,24.736%20C37.888,24.224%2037.472,23.808%2036.96,23.808%20C36.464,23.808%2036.032,24.224%2036.032,24.736%20C36.032,25.248%2036.464,25.648%2036.96,25.648%20Z%20M36.256,34.672%20L37.696,34.672%20L37.696,26.944%20L36.256,26.944%20L36.256,34.672%20Z%22%20id=%22i%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M39.984,34.672%20L41.424,34.672%20L41.424,29.296%20C41.76,28.72%2042.736,28.176%2043.456,28.176%20C43.648,28.176%2043.808,28.192%2043.952,28.224%20L43.952,26.768%20C42.928,26.768%2042.016,27.36%2041.424,28.128%20L41.424,26.944%20L39.984,26.944%20L39.984,34.672%20Z%22%20id=%22r%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M45.232,36.4%20L45.008,37.696%20C45.232,37.76%2045.664,37.808%2045.904,37.808%20C47.024,37.792%2047.872,37.36%2048.368,36.144%20L52.176,26.944%20L50.624,26.944%20L48.208,33.008%20L45.792,26.944%20L44.256,26.944%20L47.44,34.752%20L46.992,35.776%20C46.752,36.352%2046.4,36.528%2045.872,36.528%20C45.68,36.528%2045.408,36.48%2045.232,36.4%20Z%22%20id=%22y%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%3C/g%3E%3C/svg%3E "ICT Button Desktop")
%3C/title%3E%20%20%20%20%3Cg%20id=%22ICT-Button-(768)%22%20stroke=%22none%22%20stroke-width=%221%22%20fill=%22none%22%20fill-rule=%22evenodd%22%3E%20%20%20%20%20%20%20%20%3Cg%20id=%22ICT-Button%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M0,0%20L77,0%20L77,86%20L16,86%20C7.163444,86%208.18759336e-15,78.836556%200,70%20L0,0%20L0,0%20Z%22%20id=%22Rectangle%22%20fill=%22%23231F20%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cg%20id=%22Make-an-Enquiry%22%20transform=%22translate(12.888000,%2042.996000)%22%20fill=%22%23FFFFFF%22%20fill-rule=%22nonzero%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22M%22%20points=%226.888%208.004%208.088%208.004%208.088%200%206.372%200%204.044%205.748%201.716%200%200%200%200%208.004%201.2%208.004%201.2%201.644%203.792%208.004%204.296%208.004%206.888%201.644%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M13.416,8.004%20L14.496,8.004%20L14.496,4.092%20C14.496,2.616%2013.428,2.064%2012.168,2.064%20C11.232,2.064%2010.44,2.376%209.792,3.012%20L10.26,3.756%20C10.776,3.24%2011.34,2.988%2012,2.988%20C12.828,2.988%2013.416,3.42%2013.416,4.14%20L13.416,5.1%20C12.972,4.584%2012.3,4.332%2011.52,4.332%20C10.548,4.332%209.504,4.908%209.504,6.228%20C9.504,7.5%2010.56,8.148%2011.52,8.148%20C12.3,8.148%2012.96,7.872%2013.416,7.368%20L13.416,8.004%20Z%20M13.416,6.732%20C13.092,7.164%2012.528,7.392%2011.928,7.392%20C11.148,7.392%2010.596,6.924%2010.596,6.24%20C10.596,5.556%2011.148,5.088%2011.928,5.088%20C12.528,5.088%2013.092,5.316%2013.416,5.748%20L13.416,6.732%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22k%22%20points=%2220.112%208.004%2021.48%208.004%2018.96%204.836%2021.456%202.208%2020.1%202.208%2017.304%205.148%2017.304%200%2016.224%200%2016.224%208.004%2017.304%208.004%2017.304%206.396%2018.18%205.508%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M22.104,5.1%20C22.104,6.924%2023.376,8.148%2025.104,8.148%20C26.04,8.148%2026.856,7.848%2027.432,7.284%20L26.928,6.576%20C26.496,7.02%2025.824,7.26%2025.212,7.26%20C24.048,7.26%2023.328,6.444%2023.244,5.46%20L27.828,5.46%20L27.828,5.196%20C27.828,3.42%2026.748,2.064%2025.008,2.064%20C23.316,2.064%2022.104,3.42%2022.104,5.1%20Z%20M25.008,2.952%20C26.232,2.952%2026.748,3.912%2026.772,4.68%20L23.232,4.68%20C23.292,3.888%2023.844,2.952%2025.008,2.952%20Z%22%20id=%22e%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M35.856,8.004%20L36.936,8.004%20L36.936,4.092%20C36.936,2.616%2035.868,2.064%2034.608,2.064%20C33.672,2.064%2032.88,2.376%2032.232,3.012%20L32.7,3.756%20C33.216,3.24%2033.78,2.988%2034.44,2.988%20C35.268,2.988%2035.856,3.42%2035.856,4.14%20L35.856,5.1%20C35.412,4.584%2034.74,4.332%2033.96,4.332%20C32.988,4.332%2031.944,4.908%2031.944,6.228%20C31.944,7.5%2033,8.148%2033.96,8.148%20C34.74,8.148%2035.4,7.872%2035.856,7.368%20L35.856,8.004%20Z%20M35.856,6.732%20C35.532,7.164%2034.968,7.392%2034.368,7.392%20C33.588,7.392%2033.036,6.924%2033.036,6.24%20C33.036,5.556%2033.588,5.088%2034.368,5.088%20C34.968,5.088%2035.532,5.316%2035.856,5.748%20L35.856,6.732%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M42.576,8.004%20L43.656,8.004%20L43.656,3.936%20C43.656,2.712%2043.02,2.064%2041.796,2.064%20C40.896,2.064%2040.128,2.556%2039.744,3.024%20L39.744,2.208%20L38.664,2.208%20L38.664,8.004%20L39.744,8.004%20L39.744,3.864%20C40.056,3.432%2040.668,3.024%2041.34,3.024%20C42.084,3.024%2042.576,3.336%2042.576,4.296%20L42.576,8.004%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22E%22%20points=%220%2026.004%205.376%2026.004%205.376%2024.948%201.2%2024.948%201.2%2022.452%205.292%2022.452%205.292%2021.396%201.2%2021.396%201.2%2019.056%205.376%2019.056%205.376%2018%200%2018%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M10.764,26.004%20L11.844,26.004%20L11.844,21.936%20C11.844,20.712%2011.208,20.064%209.984,20.064%20C9.084,20.064%208.316,20.556%207.932,21.024%20L7.932,20.208%20L6.852,20.208%20L6.852,26.004%20L7.932,26.004%20L7.932,21.864%20C8.244,21.432%208.856,21.024%209.528,21.024%20C10.272,21.024%2010.764,21.336%2010.764,22.296%20L10.764,26.004%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M18.768,28.212%20L18.768,20.208%20L17.688,20.208%20L17.688,21.036%20C17.256,20.46%2016.56,20.064%2015.78,20.064%20C14.268,20.064%2013.2,21.204%2013.2,23.1%20C13.2,24.996%2014.268,26.148%2015.78,26.148%20C16.536,26.148%2017.22,25.8%2017.688,25.164%20L17.688,28.212%20L18.768,28.212%20Z%20M17.688,24.336%20C17.388,24.792%2016.728,25.188%2016.08,25.188%20C15,25.188%2014.328,24.312%2014.328,23.1%20C14.328,21.9%2015,21.024%2016.08,21.024%20C16.728,21.024%2017.388,21.408%2017.688,21.876%20L17.688,24.336%20Z%22%20id=%22q%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M24.396,26.004%20L25.476,26.004%20L25.476,20.208%20L24.396,20.208%20L24.396,24.372%20C24.072,24.804%2023.46,25.188%2022.788,25.188%20C22.044,25.188%2021.564,24.9%2021.564,23.94%20L21.564,20.208%20L20.484,20.208%20L20.484,24.3%20C20.484,25.524%2021.096,26.148%2022.332,26.148%20C23.22,26.148%2023.952,25.692%2024.396,25.212%20L24.396,26.004%20Z%22%20id=%22u%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M27.72,19.236%20C28.104,19.236%2028.416,18.936%2028.416,18.552%20C28.416,18.168%2028.104,17.856%2027.72,17.856%20C27.348,17.856%2027.024,18.168%2027.024,18.552%20C27.024,18.936%2027.348,19.236%2027.72,19.236%20Z%20M27.192,26.004%20L28.272,26.004%20L28.272,20.208%20L27.192,20.208%20L27.192,26.004%20Z%22%20id=%22i%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M29.988,26.004%20L31.068,26.004%20L31.068,21.972%20C31.32,21.54%2032.052,21.132%2032.592,21.132%20C32.736,21.132%2032.856,21.144%2032.964,21.168%20L32.964,20.076%20C32.196,20.076%2031.512,20.52%2031.068,21.096%20L31.068,20.208%20L29.988,20.208%20L29.988,26.004%20Z%22%20id=%22r%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M33.924,27.3%20L33.756,28.272%20C33.924,28.32%2034.248,28.356%2034.428,28.356%20C35.268,28.344%2035.904,28.02%2036.276,27.108%20L39.132,20.208%20L37.968,20.208%20L36.156,24.756%20L34.344,20.208%20L33.192,20.208%20L35.58,26.064%20L35.244,26.832%20C35.064,27.264%2034.8,27.396%2034.404,27.396%20C34.26,27.396%2034.056,27.36%2033.924,27.3%20Z%22%20id=%22y%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cg%20id=%22accordion-plus%22%20transform=%22translate(12.000000,%2012.000000)%22%20fill=%22%23FFFFFF%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22Shape%22%20points=%2216%207.61904762%208.38095238%207.61904762%208.38095238%200%207.61904762%200%207.61904762%207.61904762%200%207.61904762%200%208.38095238%207.61904762%208.38095238%207.61904762%2016%208.38095238%2016%208.38095238%208.38095238%2016%208.38095238%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%3C/g%3E%3C/svg%3E "ICT Button Tablet")
%3C/title%3E%20%20%20%20%3Cg%20id=%22ICT-Button-(375)%22%20stroke=%22none%22%20stroke-width=%221%22%20fill=%22none%22%20fill-rule=%22evenodd%22%3E%20%20%20%20%20%20%20%20%3Cg%20id=%22ICT-Button%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M0,0%20L60,0%20L60,72%20L12,72%20C5.372583,72%208.11624501e-16,66.627417%200,60%20L0,0%20L0,0%20Z%22%20id=%22Rectangle%22%20fill=%22%23231F20%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cg%20id=%22accordion-plus%22%20transform=%22translate(10.000000,%2010.000000)%22%20fill=%22%23FFFFFF%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22Shape%22%20points=%2212%205.71428571%206.28571429%205.71428571%206.28571429%200%205.71428571%200%205.71428571%205.71428571%200%205.71428571%200%206.28571429%205.71428571%206.28571429%205.71428571%2012%206.28571429%2012%206.28571429%206.28571429%2012%206.28571429%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%20%20%20%20%3Cg%20id=%22Make-an-Enquiry%22%20transform=%22translate(10.740000,%2034.330000)%22%20fill=%22%23FFFFFF%22%20fill-rule=%22nonzero%22%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22M%22%20points=%225.74%206.67%206.74%206.67%206.74%200%205.31%200%203.37%204.79%201.43%200%200%200%200%206.67%201%206.67%201%201.37%203.16%206.67%203.58%206.67%205.74%201.37%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M11.18,6.67%20L12.08,6.67%20L12.08,3.41%20C12.08,2.18%2011.19,1.72%2010.14,1.72%20C9.36,1.72%208.7,1.98%208.16,2.51%20L8.55,3.13%20C8.98,2.7%209.45,2.49%2010,2.49%20C10.69,2.49%2011.18,2.85%2011.18,3.45%20L11.18,4.25%20C10.81,3.82%2010.25,3.61%209.6,3.61%20C8.79,3.61%207.92,4.09%207.92,5.19%20C7.92,6.25%208.8,6.79%209.6,6.79%20C10.25,6.79%2010.8,6.56%2011.18,6.14%20L11.18,6.67%20Z%20M11.18,5.61%20C10.91,5.97%2010.44,6.16%209.94,6.16%20C9.29,6.16%208.83,5.77%208.83,5.2%20C8.83,4.63%209.29,4.24%209.94,4.24%20C10.44,4.24%2010.91,4.43%2011.18,4.79%20L11.18,5.61%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22k%22%20points=%2216.76%206.67%2017.9%206.67%2015.8%204.03%2017.88%201.84%2016.75%201.84%2014.42%204.29%2014.42%200%2013.52%200%2013.52%206.67%2014.42%206.67%2014.42%205.33%2015.15%204.59%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M18.42,4.25%20C18.42,5.77%2019.48,6.79%2020.92,6.79%20C21.7,6.79%2022.38,6.54%2022.86,6.07%20L22.44,5.48%20C22.08,5.85%2021.52,6.05%2021.01,6.05%20C20.04,6.05%2019.44,5.37%2019.37,4.55%20L23.19,4.55%20L23.19,4.33%20C23.19,2.85%2022.29,1.72%2020.84,1.72%20C19.43,1.72%2018.42,2.85%2018.42,4.25%20Z%20M20.84,2.46%20C21.86,2.46%2022.29,3.26%2022.31,3.9%20L19.36,3.9%20C19.41,3.24%2019.87,2.46%2020.84,2.46%20Z%22%20id=%22e%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M29.88,6.67%20L30.78,6.67%20L30.78,3.41%20C30.78,2.18%2029.89,1.72%2028.84,1.72%20C28.06,1.72%2027.4,1.98%2026.86,2.51%20L27.25,3.13%20C27.68,2.7%2028.15,2.49%2028.7,2.49%20C29.39,2.49%2029.88,2.85%2029.88,3.45%20L29.88,4.25%20C29.51,3.82%2028.95,3.61%2028.3,3.61%20C27.49,3.61%2026.62,4.09%2026.62,5.19%20C26.62,6.25%2027.5,6.79%2028.3,6.79%20C28.95,6.79%2029.5,6.56%2029.88,6.14%20L29.88,6.67%20Z%20M29.88,5.61%20C29.61,5.97%2029.14,6.16%2028.64,6.16%20C27.99,6.16%2027.53,5.77%2027.53,5.2%20C27.53,4.63%2027.99,4.24%2028.64,4.24%20C29.14,4.24%2029.61,4.43%2029.88,4.79%20L29.88,5.61%20Z%22%20id=%22a%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M35.48,6.67%20L36.38,6.67%20L36.38,3.28%20C36.38,2.26%2035.85,1.72%2034.83,1.72%20C34.08,1.72%2033.44,2.13%2033.12,2.52%20L33.12,1.84%20L32.22,1.84%20L32.22,6.67%20L33.12,6.67%20L33.12,3.22%20C33.38,2.86%2033.89,2.52%2034.45,2.52%20C35.07,2.52%2035.48,2.78%2035.48,3.58%20L35.48,6.67%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpolygon%20id=%22E%22%20points=%220%2022.67%204.48%2022.67%204.48%2021.79%201%2021.79%201%2019.71%204.41%2019.71%204.41%2018.83%201%2018.83%201%2016.88%204.48%2016.88%204.48%2016%200%2016%22%3E%3C/polygon%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M8.97,22.67%20L9.87,22.67%20L9.87,19.28%20C9.87,18.26%209.34,17.72%208.32,17.72%20C7.57,17.72%206.93,18.13%206.61,18.52%20L6.61,17.84%20L5.71,17.84%20L5.71,22.67%20L6.61,22.67%20L6.61,19.22%20C6.87,18.86%207.38,18.52%207.94,18.52%20C8.56,18.52%208.97,18.78%208.97,19.58%20L8.97,22.67%20Z%22%20id=%22n%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M15.64,24.51%20L15.64,17.84%20L14.74,17.84%20L14.74,18.53%20C14.38,18.05%2013.8,17.72%2013.15,17.72%20C11.89,17.72%2011,18.67%2011,20.25%20C11,21.83%2011.89,22.79%2013.15,22.79%20C13.78,22.79%2014.35,22.5%2014.74,21.97%20L14.74,24.51%20L15.64,24.51%20Z%20M14.74,21.28%20C14.49,21.66%2013.94,21.99%2013.4,21.99%20C12.5,21.99%2011.94,21.26%2011.94,20.25%20C11.94,19.25%2012.5,18.52%2013.4,18.52%20C13.94,18.52%2014.49,18.84%2014.74,19.23%20L14.74,21.28%20Z%22%20id=%22q%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M20.33,22.67%20L21.23,22.67%20L21.23,17.84%20L20.33,17.84%20L20.33,21.31%20C20.06,21.67%2019.55,21.99%2018.99,21.99%20C18.37,21.99%2017.97,21.75%2017.97,20.95%20L17.97,17.84%20L17.07,17.84%20L17.07,21.25%20C17.07,22.27%2017.58,22.79%2018.61,22.79%20C19.35,22.79%2019.96,22.41%2020.33,22.01%20L20.33,22.67%20Z%22%20id=%22u%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M23.1,17.03%20C23.42,17.03%2023.68,16.78%2023.68,16.46%20C23.68,16.14%2023.42,15.88%2023.1,15.88%20C22.79,15.88%2022.52,16.14%2022.52,16.46%20C22.52,16.78%2022.79,17.03%2023.1,17.03%20Z%20M22.66,22.67%20L23.56,22.67%20L23.56,17.84%20L22.66,17.84%20L22.66,22.67%20Z%22%20id=%22i%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M24.99,22.67%20L25.89,22.67%20L25.89,19.31%20C26.1,18.95%2026.71,18.61%2027.16,18.61%20C27.28,18.61%2027.38,18.62%2027.47,18.64%20L27.47,17.73%20C26.83,17.73%2026.26,18.1%2025.89,18.58%20L25.89,17.84%20L24.99,17.84%20L24.99,22.67%20Z%22%20id=%22r%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%20%3Cpath%20d=%22M28.27,23.75%20L28.13,24.56%20C28.27,24.6%2028.54,24.63%2028.69,24.63%20C29.39,24.62%2029.92,24.35%2030.23,23.59%20L32.61,17.84%20L31.64,17.84%20L30.13,21.63%20L28.62,17.84%20L27.66,17.84%20L29.65,22.72%20L29.37,23.36%20C29.22,23.72%2029,23.83%2028.67,23.83%20C28.55,23.83%2028.38,23.8%2028.27,23.75%20Z%22%20id=%22y%22%3E%3C/path%3E%20%20%20%20%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%20%20%20%20%3C/g%3E%20%20%20%20%3C/g%3E%3C/svg%3E "ICT Button Mobile")
Why Are Frown Lines Traditionally Treated With Five Injection Points?
This article is provided for general educational purposes only. It is not intended to promote a specific treatment or technique, nor to replace an individual consultation with a qualified medical practitioner. Treatment approaches vary and should always be tailored to the individual following a clinical assessment.
Anti-wrinkle injections for frown lines — the vertical lines between the eyebrows — are among the most commonly performed cosmetic procedures worldwide. Despite this, many patients are surprised to learn that the technique used to treat this area is often remarkably uniform.
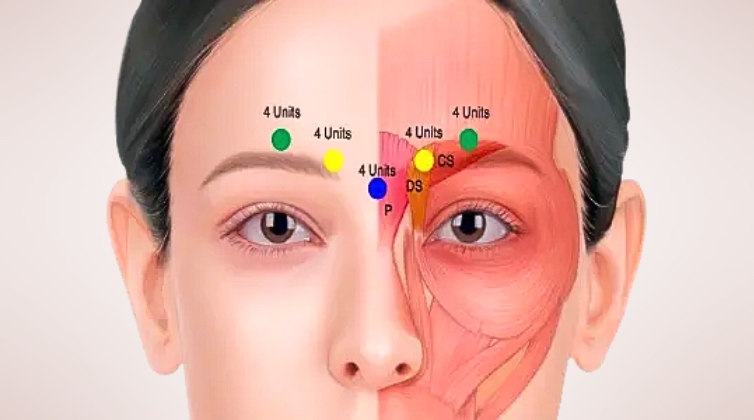
In many clinics, frown lines are treated using a five-point injection pattern — the same diagram, repeated across many different faces.
So where did this approach come from?
And is it really designed around individual facial anatomy?
The Origin of the 5-Point Frown Line Technique
The traditional five-point injection pattern did not arise from facial anatomy textbooks or personalised treatment philosophy. Instead, it originates from the original clinical trials used to obtain regulatory approval for botulinum toxin type A for cosmetic use.
In 2002, Botox Cosmetic was approved by the U.S. Food and Drug Administration (FDA) for the temporary improvement of moderate to severe glabellar lines (frown lines). To conduct these trials, researchers needed:
- A standardised dose
- A repeatable injection pattern
- A method that could be applied consistently across large patient groups
As a result, the trial protocol used:
- A total dose of 20 units
- Delivered across five fixed injection points
- Targeting the corrugator supercilii and procerus muscles
This approach allowed outcomes to be measured reliably. However, it was designed for research consistency, not individual facial variation.
Over time, this trial diagram became widely taught and adopted as the default method in clinical practice.
What the Approval Trials Did — and Did Not — Examine
The original FDA approval trials demonstrated that botulinum toxin could safely and effectively reduce the appearance of frown lines when used as studied. However, it is important to understand their limitations.
These trials did not compare:
- Different numbers of injection points
- Smaller versus larger injections
- Deeper versus more superficial placement
- Personalised muscle mapping versus fixed diagrams
In other words, the five-point technique was the method studied, not necessarily the most anatomically precise or flexible approach.
Understanding Frown Line Anatomy
Frown lines are primarily produced by two muscles:
- Corrugator supercilii — paired muscles that draw the eyebrows inward and downward
- Procerus — a midline muscle that contributes to horizontal lines over the nasal bridge
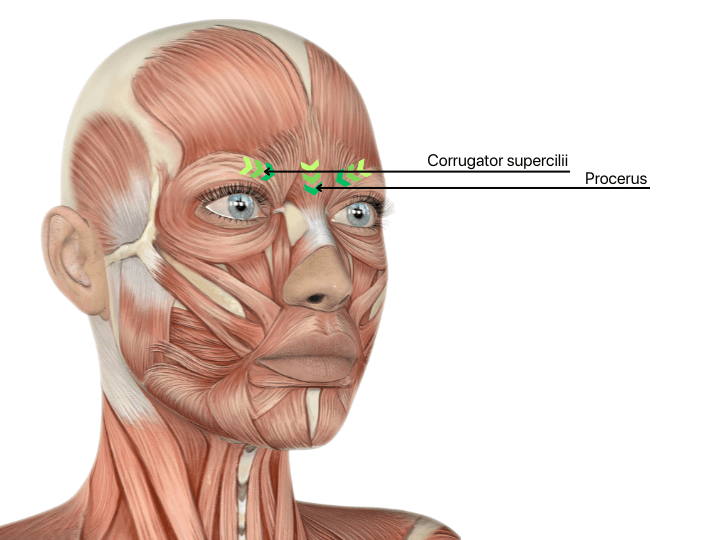
The corrugator muscle is often misunderstood. Rather than being a short, straight structure, it is:
- Fan-shaped
- Variable in size and strength
- Extending further laterally than many diagrams suggest
- Thinner and more superficial as it approaches the eyebrow
Crucially, this anatomy varies between individuals. No two corrugator muscles are identical.
A fixed injection map cannot fully account for these differences.
What We Know About Toxin Spread (Diffusion)
Scientific research and regulatory labelling consistently acknowledge that botulinum toxin can spread beyond the exact injection site. This phenomenon — often referred to as diffusion or spread — is influenced by several factors, including:
- Injection volume
- Dose per injection point
- Depth of placement
- Local tissue characteristics
In simple terms:
- Larger volumes tend to spread further
- Smaller, more precise injections are more localised
This is particularly relevant in the glabellar region because of the proximity of muscles involved in eyelid elevation and brow support.
Injection Depth Matters — Especially From Lateral to Medial
One of the more nuanced aspects of glabellar anatomy is that muscle depth changes across the frown region.
- Medially (closer to the centre of the face), the corrugator muscle lies deeper, closer to bone.
- Laterally (toward the eyebrow), the muscle becomes thinner and more superficial as it approaches the orbital rim.
Beneath the lateral brow region are anatomical pathways associated with the levator palpebrae superioris muscle, which is responsible for lifting the upper eyelid.
Because of this, unintended spread of toxin in the lateral glabellar area may increase the risk of eyelid heaviness or drooping.
From an anatomical and diffusion perspective, many practitioners therefore consider:
- More superficial placement laterally, where the muscle is thinner
- Deeper placement medially, where the muscle bulk is greater and further from eyelid-elevating structures
This gradient in depth — superficial laterally, deeper medially — reflects anatomy rather than a fixed diagram.
Why Some Practitioners Use More Than 5 Injection Points
Because the corrugator muscle changes in shape, thickness, and depth from lateral to medial, some modern approaches use more injection points with smaller amounts.
The rationale is not to use more product, but to:
- Match the natural contour of the muscle
- Allow depth to vary gradually across the region
- Reduce reliance on larger single injections
- Improve precision while limiting unintended spread
It is important to emphasise that this reflects clinical judgment informed by anatomy and diffusion principles, rather than a universally proven “best” method. To date, there are no large comparative trials directly evaluating different injection-point patterns.
A Shift Toward Individualised Frown Lines Treatment
Cosmetic medicine continues to evolve. While early regulatory trials established safety and efficacy, modern practice increasingly recognises that:
- Facial anatomy varies widely
- High-risk areas require careful planning
- Technique matters as much as dose
- Personalisation plays an important role in natural outcomes
Understanding where commonly taught techniques come from allows patients to engage in more informed discussions about treatment planning, anatomy, and safety.
In Summary
- The traditional five-point frown line injection pattern originates from early FDA approval trials
- It was designed for research standardisation, not individual anatomy
- The corrugator muscle varies significantly between individuals
- Scientific evidence shows that injection volume and depth influence toxin spread
- Anatomical considerations suggest that depth may vary from lateral to medial
- Some practitioners adapt their techniques to reflect these principles
Cosmetic treatments are most effective and safest when grounded in anatomy, evidence, and thoughtful clinical assessment — rather than rigid diagrams alone.